JacketFlap connects you to the work of more than 200,000 authors, illustrators, publishers and other creators of books for Children and Young Adults. The site is updated daily with information about every book, author, illustrator, and publisher in the children's / young adult book industry. Members include published authors and illustrators, librarians, agents, editors, publicists, booksellers, publishers and fans. Join now (it's free).
Login or Register for free to create your own customized page of blog posts from your favorite blogs. You can also add blogs by clicking the "Add to MyJacketFlap" links next to the blog name in each post.
Blog Posts by Tag
In the past 7 days
Blog Posts by Date
Click days in this calendar to see posts by day or month
Viewing: Blog Posts Tagged with: Ebola, Most Recent at Top [Help]
Results 1 - 24 of 24
How to use this Page
You are viewing the most recent posts tagged with the words: Ebola in the JacketFlap blog reader. What is a tag? Think of a tag as a keyword or category label. Tags can both help you find posts on JacketFlap.com as well as provide an easy way for you to "remember" and classify posts for later recall. Try adding a tag yourself by clicking "Add a tag" below a post's header. Scroll down through the list of Recent Posts in the left column and click on a post title that sounds interesting. You can view all posts from a specific blog by clicking the Blog name in the right column, or you can click a 'More Posts from this Blog' link in any individual post.
After the West African Ebola epidemic of 2014, hardly anyone contests that the World Health Organization (WHO) made fatal mistakes during the crisis. It reacted too late and did too little to contain the outbreak before it got out of control. And it once again exposed its deeply entrenched dysfunctions that make it so difficult for the organization to live up to its role as the central standard setter, coordinator and crisis manager in global health
‘Ebola is a wake-up call.’ This is a common sentiment expressed by those who have reflected on the ongoing Ebola outbreak in West Africa. It is a reaction to the nearly 30,000 cases and over 11,000 deaths that have occurred since the first cases of the outbreak were reported in March 2014.
The date-line is 2014. An outbreak of a deadly disease in a remote region, beyond the borders of a complacent Europe. Local deaths multiply. The risk does not end with death, either, because corpses hold the highest risk of contamination and you must work to contain their threat. All this is barely even reported at first, until the health of a Western visitor, a professional man, breaks down.
As Ebola recedes from the headlines, amid long awaited declines in incidence in West Africa, a long overdue commitment to developing vaccines and adequate health care infrastructure is underway. The importance of these approaches should not to be minimized.
Last year was an important year in the field of public health. In 2014, West Africa, particularly Sierra Leone, Liberia, and Guinea, experienced the worst outbreak of the Ebola virus in history, and with devastating effects. Debates around e-cigarettes and vaping became central, as more research was published about their health implications. Conversations surrounding nutrition and the spread of disease through travel and migration continued in the media and among experts.
We’ve chosen a selection of articles that discuss public health issues that arose in 2014, their effects on the present and implications for the future.
Header image: US specialist helping Afghan nomads by Sfc. Larry Johns (US Army). Public domain via Wikimedia Commons.
Many in the media and academia (myself included) have been discussing the Ebola crisis, and more specifically, the issues that arise as Ebola has traveled with infected patients and health care workers to the United States and infected other US citizens.
These discussions have been fascinating and frightening, but the terrifying truth is that Ebola is just the tip of the iceberg. Diseases have long traveled with patients, and as the phenomena of medical tourism and the more general globalization of health care grow, these problems are likely to grow as well.
Medical tourists are very good targets of opportunities for pathogens. Many are traveling with compromised or suppressed immune systems to destination countries for treatment with relatively high infection rates, including the risk of exposure to multi-drug–resistant pathogens.
Doctors typically distinguish commensals—the bugs we normally carry on our skin, mouth, digestive tracts, etc.—from pathogens, the harmful bacteria that cause disease through infection. But what is commensal for a person in India might be an exotic pathogen for a US population. Medical tourist patients are transporting their commensals and pathogens to the hospital environments of the destination countries to which they travel, and are exposed to the commensals and pathogens of hospitals and population at large in the destination country. These transmissions tax the health care system and the knowledge of physicians in the home country to whom the new microbe may be unknown, and diagnosis and treatment more difficult.
Air travel can involve each of the four classical modes of disease transmission: contact (e.g. body-to-body or touching an armrest), common vehicle (e.g. via food or water), vector (e.g. via insects or vermin), and airborne (although more recent planes are equipped with high efficiency particulate air (HEPA) filters reducing transmission risk, older planes are not).
We have seen several diseases travel in this way. The Severe Acute Respiratory Syndrome (SARS) outbreak of 2003 involved a three-hour flight from Hong Kong to Beijing carrying one SARS-infected passenger leading to sixteen passengers being subsequently confirmed as cases of SARS, with eight of those passengers sitting in the three rows in front of the passenger.
In January 2008, a new type of enzyme was detected in bacteria found in a fifty-nine-year-old man with a urinary tract infection being treated in Sweden. The man, Swedish but of Indian origin, had in the previous month undergone surgeries at two hospitals in India. The enzyme, labeled “New Delhi metallo-beta-lactamase-1 (NDM-1)” was able to disarm a lot of antibiotics, including one that was the last line of defenses against common respiratory and urinary tract infection.
In 2009, a study found that twenty-nine UK patients had tested positive for the bacteria-carrying NDM-1 and that seventeen of the twenty-nine (60%) had traveled to India or Pakistan in the year before. A majority of those seventeen received medical treatment while abroad in those countries, some for accidents or illness while traveling and others for medical tourism, either for kidney and bone marrow transplants or for cosmetic surgery.
High-income countries face significant problems with these infections. A 2002 study estimated that 1.7 million patients (ninety-nine thousand of whom died as a result) developed health care-acquired infections in the United States that year. In Europe these infections have been estimated to cause thirty-seven thousand deaths a year and add US $9.4 billion in direct costs
What can be done? Although in theory airline or national travel rules can prevent infected patients from boarding planes, detecting these infections in passengers is very difficult for the airline or immigration officials, and concerns about privacy of patients may chill some interventions. A 2007 case of a man who flew from the United States to Europe with extensively resistant tuberculosis and who ultimately circumvented authorities who tried to stop him on return by flying to Montreal, Canada and renting a car, shows some of the limits on these restrictions.
Part of the solution is technological. The HEPA filters discussed above on newer model planes reduce the risk substantially, and we can hope for more breakthroughs.
Part of the solution is better regulating the use of antibiotics: overuse of antibiotics when not effective or necessary, underuse of antibiotics when they are needed, failure to complete a full course of antibiotics, counterfeit drugs, and excessive antibiotic use in food animals. This is not a magic bullet, however, and we see problems even in countries with prescription systems such as the United States.
We also need much better transparency and reaction time. Some countries reacted quickly to the report of the NDM-1 cases discussed above in issuing travel warnings and informing home country physicians, while others did not.
Finally, as became evident with Ebola, we need better protocols in place to screen returning medical tourism patients and to engage in infection control when needed.
Headline image credit: Ebola virus virion by CDC microbiologist Cynthia Goldsmith. Public domain via Wikimedia Commons.
Although the number of Ebola cases and deaths has jumped dramatically in the short time since we wrote our December Briefing on the epidemic, there are signs of hope. Ebola is slowing down in areas where there was previously high transmission, in Liberia and in Eastern Sierra Leone for example. The lesson from past Ebola epidemics is that learning and local adaptation has played a central role in controlling previous outbreaks; now in West Africa the curve of the epidemic seems to be turning as people alter their behaviour. The apparent avoidance of continued exponential growth is a relief but it is no cause for complacency.
Freetown and the North of Sierra Leone are still suffering heavily. There is likely to be ongoing transmission for some time with sporadic clusters of cases as the epidemic moves into its next phase. The message, that local people should be involved and that their perspectives and knowledge are both valid and valuable, is still essential. Now is the time to find a balance between medical interventions, emergency thinking, and more humane and localised approaches based on collaboration.
As and when the epidemic ends, there should also be no complacency about the structural violence which produced this crisis. Structural violence refers to the way institutions and practices inflict avoidable harm by impairing basic human needs. The long term view — which locates this epidemic in the context of economic, social, technical, discursive and political exclusions and injustices — needs to be at the forefront of recovery and ‘development’ post-Ebola. The stark evidence of violence, in the form of distrust, the collapse of already dysfunctional health services, the catastrophic costs of Ebola on families and countries, the unpaid salaries of nurses and burial teams, the lack of protection – whether in the form of plastic gloves or welfare nets in times of crisis – must not fade with a return to business as usual. The Ebola crisis should be a game-changer for development.
In pointing to structural violence, we aren’t talking of a single social institution, but of overlapping institutions and practices that have produced interlocking inequalities, unsustainabilities, and insecurities. Aid and development have failed to address these conditions. Sierra Leone and Liberia attract considerable foreign direct investment and record some of the world’s highest growth figures yet most of their populations live in continued or worsening poverty. The emerging field of global health emphasizes networks and shared vulnerabilities, but in practice — through disjointed programmes and a tendency towards ‘quick wins’ — has neglected dire inequalities, which mean a virus like Ebola can tear a country up due to an absence of the most fundamental public health and state capacities. These structural and related socio-cultural conditions are not quickly or easily addressed, but Ebola has highlighted how vast disparities, internationally and within countries, are not sustainable. A greater focus on inclusive institutions and economies, and on conceiving of health as a global public good, is needed in order to build trust and resilience. Achieving that will involve asking difficult questions about aid and development as practiced in this region.
Both the crisis response and efforts to address its structural underpinnings are strengthened by recognition of the complex and historically-embedded logics and relationships which shape people’s lives. The Ebola Response Anthropology Platform has been set up to network anthropologists and other social scientists across the world with fieldworkers and communities, and to provide an interface with those planning and implementing the Ebola response so that such perspectives can be integrated into the response. Complementary initiatives, like one supported by the American Anthropological Association, mean that there is now a groundswell of debate and commentary on these critical dimensions. Much of this is building on research conducted over decades of post-colonial development and post-conflict reconstruction that, with the benefit of hindsight, is revealing of the fault-lines of the Ebola epidemic. As ‘the response’ transitions into another phase of reconstruction it is critical that these lessons, and the complexities they reveal, are fully appreciated to prevent further disasters for this region.
Headline image credit: Conakry, Guinea, 2011. Photo by CDC Global. CC BY 2.0 via Flickr.
How did the international community get the response to the Ebola outbreak so wrong? We closed borders. We created panic. We left the moribund without access to health care. When governments in Liberia, Sierra Leone, Senegal, Guinea, Mali, and Nigeria called out to the world for help, the global response went to mostly protect the citizens of wealthy nations before strengthening health systems on the ground. In general, resources have gone to guarding borders rather than protecting patients in the hot zone from the virus. Yet, Cuba broke this trend by sending in hundreds of its own health workers into the source of the epidemic. Considering the broader global response to Ebola, why did Cuba get it so right?
Ebola impacted countries, and the World Health Organization (WHO), called out for greater human resources for health. While material supplies arrived, many countries tightened travel restrictions, closed their doors and kept their medical personnel at home. At a time when there has never been greater knowledge, more money, and ample resources for global health, the world responded to an infectious pathogen with some material supplies, but also with securitization, experimental vaccines, and forced quarantines – all of which oppose accepted public health ethics. The result is that without human resources for health on the ground, the supplies stay idle, the vaccines remain questionable, and the securitization instills fear.
The Global North evacuated their infected citizens. These evacuations spawned donations to the WHO and then led to travel bans. The United Kingdom provided £230 million in material aid to West Africa. The United States committed $175 million to combat the virus by transporting supplies and personnel, with an estimated 3,000 soldiers to be involved in the response. Canada’s government provided some $35 million to Ebola, including a mobile testing lab, sanitary equipment and 1,000 vials of experimental vaccines that have yet to arrive in West Africa or even be tested on humans. Canada then followed the example of Australia, North Korea, and other nervous nations, in imposing a visa ban on persons traveling from Ebola affected countries. Even Rwanda imposed screening on Americans because of confirmed cases in the United States.
Despite this global trend, Cuba — a small and economically hobbled nation — chose to make a world of difference for those suffering from Ebola by sending in 465 health workers, expanding hospital beds, and training local health workers on how to treat and prevent the virus. Cuba is the only nation to respond to the call to stop the Ebola epidemic by actually scaling up health care capacity in the very places where it is needed the most. Even with a Gross Domestic Product per capita to that of Montenegro, Cuba has proven itself as a global health power during the 2014 Ebola outbreak. Many scholars and pundits have been left wondering not only how a low-income country, with its own social and economic challenges, could send impressive medical resources to West Africa, but also why they would dive into the hot zone in the first place — especially when nobody else dares to do so.
Cuba is globally recognized as an outstanding health-care power in providing affordable and accessible health services to its own citizens and to the citizens of 76 countries around the world, including those impacted by Ebola. Cuba’s health outreach is grounded in the epistemology of solidarity — a normative approach to global health that offers a unique ability of strengthening the core of health systems through long-term commitments to health promotion, disease prevention and primary care. Solidarity is a cooperative relationship between two parties that is mutually transformative by maximizing health-care provision, eroding power structures that promote inequity, and by seeking out mutual social and economic benefit. The reason for the general amazement and wonder over Cuba’s Ebola-response stems from a lack of depth in understanding the normative values of solidarity, as it is not a driving force in the global health outreach by most wealthy nations. The ethic of solidarity can even be seen on the ground in West Africa with Cuban doctors like Ronald Hernandéz Torres posting photos of his Ebola team wearing the protective gear, while giving the thumbs and peace sign — an incredible snapshot of humanity that contrasts the typically frightening images of Ebola health workers.
Solidarity is not charity. Charity is governed by the will of the donor and cannot be broad enough to overcome health calamities at a systems level. Solidarity is also not pure altruism. Selfless giving is based on exceptional, and often short-term, acts for no expectation of reward or reciprocity. For Cuba, solidarity in global health comes with the expectation of cooperation, meaning that the recipient nation should offer some level of support to Cuba, be it financial or political. Solidarity also means that there is a long-term relationship to improve the strength of a health system. Cuba’s current commitment to Ebola could last months, if not years.
Cuba’s global health outreach can be approached through the lens of solidarity. This example implies engaging global health calamities with cooperation over charity, with human resources in addition to material resources, and ultimately with compassion over fear. This approach could well be at the heart of wiping out Ebola — along with every other global health calamity that continues to get the best of us because we have not yet figured out how to truly take care of each other.
“The love of my life and the father of my son came to America to marry me. It was supposed to be the first happy day of a new life of joy for us all. But before we could make our new family, he died a terrible death in a quarantined room… I am writing this book to tell people about Eric, about our love story, about our family, and about my faith that has been tested but not broken.”
These are the words of Louise Troh, whose fiancé Thomas Eric Duncan became the first man on American soil to be diagnosed with the Ebola virus, and then, the first to die of the disease in America. She will tell her story for the first time in a book to be published in April 2015 by Weinstein Books, which is a joint venture of The Weinstein Company and The Perseus Books Group.
Harvey Weinstein, co-chairman of The Weinstein Company, said, “This is a heartbreaking, emotional family story. Spanning continents and decades, Louise shows faith and grace through it all.”
According to AP, Troh says she will use part of the book proceeds for a down payment on a new home.
Since the outbreak of Ebola in Liberia, schools across the region have closed — leaving children without access to traditional education opportunities and the moral support teachers provide during times of crisis.
So when we received a call from our friends at the International Book Bank and the We Care Foundation and Library asking to include books in schooling kits they were creating, we jumped at the chance. Kids were waiting. They needed out help.
Within hours, we began a crowdfunding campaign to raise funds to send as many books as possible, with a minimum goal of $5,000.
Thanks to generous support from individuals and partners like C&S Wholesale Grocers, Lee & Low Books, The NEA Foundation, Penguin Random House and Townsend Press, we ended up raising enough funds to send more than 40,000 brand new books (with a retail value of more than $320,000) to children in Liberia.
“We know books provide educational opportunities,” said Chandler Arnold, First Book’s Chief Operating Officer, “But in times of trauma they also provide comforting bedtime stories, moments of family togetherness and the chance for children to temporarily escape from a frightening situation”
The books, now on their way to children and families in the affected area, will accompany child-focused information about preventing the spread of the disease.
“When our partner Michael Weah, director of the We-Care Foundation and Library in Monrovia, Liberia, asked us for a donation of books to be packaged up and hand-delivered to children locked out of school for a year or more due to the Ebola outbreak, we couldn’t say no,” said Brigid McDonnell, Program Director at International Book Bank. “These books not only serve as critical educational tools, but also provide entertainment and escape for kids that desperately need it. It was a pleasure for the International Book Bank to work with First Book on this donation!”
To continue to help get books to kids in need throughout the country and internationally, donate to First Book today.
Are you worried about catching the flu, or perhaps even Ebola? Just how worried should you be? Well, that depends on how fast a disease will spread over social and transportation networks, so it’s obviously important to obtain good estimates of the speed of disease transmission and to figure out good containment strategies to combat disease spread.
Diseases, rumors, memes, and other information all spread over networks. A lot of research has explored the effects of network structure on such spreading. Unfortunately, most of this research has a major issue: it considers networks that are not realistic enough, and this can lead to incorrect predictions of transmission speeds, which people are most important in a network, and so on. So how does one address this problem?
Traditionally, most studies of propagation on networks assume a very simple network structure that is static and only includes one type of connection between people. By contrast, real networks change in time — one contacts different people during weekdays and on weekends, one (hopefully) stays home when one is sick, new University students arrive from all parts of the world every autumn to settle into new cities. They also include multiple types of social ties (Facebook, Twitter, and – gasp – even face-to-face friendships), multiple modes of transportation, and so on. That is, we consume and communicate information through all sorts of channels. To consider a network with only one type of social tie ignores these facts and can potentially lead to incorrect predictions of which memes go viral and how fast information spreads. It also fails to allow differentiation between people who are important in one medium from people who are important in a different medium (or across multiple media). In fact, most real networks include a far richer “multilayer” structure. Collapsing such structures to obtain and then study a simpler network representation can yield incorrect answers for how fast diseases or ideas spread, the robustness level of infrastructures, how long it takes for interaction oscillators to synchronize, and more.
Image credit: Mobile Phone, by geralt. Public domain via Pixabay.
Recently, an increasingly large number of researchers are studying mathematical objects called “multilayer networks”. These generalize ordinary networks and allow one to incorporate time-dependence, multiple modes of connection, and other complexities. Work on multilayer networks dates back many decades in fields like sociology and engineering, and of course it is well-known that networks don’t exist in isolation but rather are coupled to other networks. The last few years have seen a rapid explosion of new theoretical tools to study multilayer networks.
And what types of things do researchers need to figure out? For one thing, it is known that multilayer structures induce correlations that are invisible if one collapses multilayer networks into simpler representations, so it is essential to figure out when and by how much such correlations increase or decrease the propagation of diseases and information, how they change the ability of oscillators to synchronize, and so on. From the standpoint of theory, it is necessary to develop better methods to measure multilayer structures, as a large majority of the tools that have been used thus far to study multilayer networks are mostly just more complicated versions of existing diagnostic and models. We need to do better. It is also necessary to systematically examine the effects of multilayer structures, such as correlations between different layers (e.g., perhaps a person who is important for the social network that is encapsulated in one layer also tends to be important in other layers?), on different types of dynamical processes. In these efforts, it is crucial to consider not only simplistic (“toy”) models — as in most of the work on multilayer networks thus far — but to move the field towards the examination of ever more realistic and diverse models and to estimate the parameters of these models from empirical data. As our review article illustrates, multilayer networks are both exciting and important to study, but the increasingly large community that is studying them still has a long way to go. We hope that our article will help steer these efforts, which promise to be very fruitful.
At first, I wasn’t sure quite why. I get what they meant. It seems like Ebola’s everywhere! It’s constantly on the news, all over the internet, and everyone’s talking about it. It makes sense to be sick of hearing about it. We’re bound to get sick of hearing about anything that much!
But still, I couldn’t shake the discomfort that rung in my head over that status. Ebola seems far away, after all, it’s only been diagnosed four times in the US. It’s easy to tuck it away in your mind as something distant that doesn’t affect you and forget why it’s a big deal.
It’s even become a hot topic for jokes on social media:
Because so many see this very real disease as a far away concept, we find safety in our distance and it’s easy to make light of it.
But guys….
4,877 deaths. 9,935 sufferers. That’s not funny. That’s not something to ask to “omg shut up.”
The idea of disease never really hit home for me until my little sister was diagnosed with cancer. Yes, Ebola and cancer are two very different things. But I know what it’s like to watch someone I love very dearly suffer. I know what it’s like to hold my sister’s hand while she cries because she can’t escape the pain or the fear that comes with her disease. I know what it’s like to cry myself to sleep begging God to take her illness away. And I can’t help but imagine a sister somewhere in Africa in a situation very similar to my own, watching her loved one suffer, hearing her cries, and begging for it to all be over- but without the blessings of medicine and technology that my sister has access to.
We are quick to throw on our pink gear for breast cancer awareness and dump ice on our head for ALS because that kind of awareness is fun and easy. I’m not trying to diminish those causes- they are great causes that deserve promotion. But I mean to make note of the fact that when another very real disease with very real consequences is brought to light and gains awareness, people groan that it’s in the news again and make jokes about it on the internet. Because Ebola doesn’t have the fun and cute promotional package, we complain and make light of it and its need for awareness and a solution.
People are suffering and dying from Ebola. Just because that suffering seems far away, doesn’t make it any less significant.
This is a guest post from my oldest daughter, Meredith. I begged her to let me post it.
If you think about big public health challenges of our day — the Ebola virus in Africa, the rising rates of suicide among the middle-aged in the United States, the HIV epidemic everywhere — religions are playing a role. When I speak, I ask audiences, “What was the first thing you heard about the Ebola crisis?”, and they always say “The missionaries who got it were taken to Emory.” “That makes my point,” I say. “You didn’t know anything about it up until that moment, but they did.” Those missionaries, and the faith-based organizations they worked for (Samaritan’s Purse and Serving in Mission) were already there on the ground along with other faith-based organizations, volunteering their time, putting their lives in danger, and providing valuable resources of equipment, supplies, and knowledgeable helping hands to try to contain the outbreak.
In another challenge, the crisis of rising suicides among US veterans and Baby Boomers, religion’s role is more in the background, but no less important. Since sociologist Emile Durkheim first studied the subject in late 19th century France, researchers have consistently found that individuals with more social ties – particularly to religious groups — are more protected from suicide. Religious ties provide caring, support, warmth, and intimacy — the “carrots” of social interaction. They also provide rules for living and guidance for behavior that often require individuals to sacrifice their self-interest for the good of the group. These are the “sticks” of social interaction, which Durkheim argued were just as necessary as the “carrots” in keeping individuals from taking their own lives. So here are two quite different roles that religions play in public health: first in the foreground, deploying resources and religious social capital as partners with public health authorities in countries around the world, and also in the background, providing the sustenance of social integration and regulation that prevents the tailspin of suicide.
But religions are complicated, and in the HIV epidemic we have seen faith traditions playing all of these roles and other less helpful ones as well. One positive thing that religions do — very effectively through religious ritual and practice — is to give individuals a sense of belonging to something larger than themselves; they bestow a social identity that marks individuals as valued members of a group, with all of that group’s rights, privileges, and responsibilities. But group membership by its very nature implies that there are other individuals and groups — outsiders — who are not members, who may be less valued. This is an obvious source of conflict around the world and can lead to violence on a small or large scale. This too, sad to say, is an instance of religions taking a role in determining the health of populations, but not in a good way. And at a less extreme level, if an individual violates the norms of the group, or breaks its rules, it can lead to sanctions, punishment, or even being cast out from membership. So in the HIV epidemic, individuals who were victimized by the disease first, in many cases experienced a secondary victimization of being stigmatized by religious groups who perceived that the disease was a sign of forbidden behaviors, and therefore a just punishment.
Public health organizations and religious organizations are both looking to promote the well-being of their communities. In many cases those interests are perfectly aligned and the two institutions function, implicitly or explicitly, as partners. When they do not, it makes sense that two powerful forces should identify all of the ways in which they can work together, finding a way around the contentious issues to leverage each other’s constructive responses. Religion, along with income inequality, education, and political structures, is one of the social determinants of public health in countries around the world, despite its usual exclusion from the public health paradigm.
Like many this past week, our attention has been fixated on the media coverage of the Ebola outbreak: images of experts showing off the proper way to put on and take off protective gloves to avoid exposure to the virus; political pundits quarrelling over the appropriateness of travel restrictions; reassuring press conferences by the director of the Centers for Disease Control. It is an event that has received immediate and intense attention and generated compelling journalism, for sure, but does it really give us an emotional understanding of the impact of the event?
What is it like for a mother or a father to watch their child die and not to be able to touch them? What happens within a community that has experienced a major outbreak? Are people brought closer through a shared suffering or are the bonds that held the community together forever broken? There are infinite questions that we could ask of the human heart in the midst or the aftermath of such an event. Oral history with its emphasis on empathy is an effective method of asking these questions.
Hopefully the epidemic will be contained, but by the time it is, it is likely that the public’s appetite for more analysis on the outbreak will have been satiated. Journalists will be compelled to move onto the new topic of the day. Oral historians, however, can — and should — linger on this event.
For oral historians, who have increasingly worked in the aftermath of crisis over the past decade, the motivation to document is fueled by both a humanitarian impulse to respond to crisis and a scholar’s desire to inquire and understand. Times of widespread crisis have an elusive complexity which defies any attempt at meta-narrative. Aspiring to get at a comprehensive picture and the countless ways in which the epidemic is impacting so many seems unfeasible. For many researchers, the most profound way to begin is to try to appreciate how this crisis manifests itself for an individual, for a family, or for a community is oral history.
Dr. Joel Montgomery, Team Lead for CDC’s Ebola Response Team in Liberia, adjusts a colleague’s protective equipment before entering the Ebola treatment unit. CDC Global. Photograph by Athalia Christie. Public domain via Flickr.
Doing oral history in West Africa in the aftermath of the epidemic will present unique challenges for interviewers. Navigating the emotional and political resonance of the Ebola outbreak will require caution, compassion, and courage, as well as flexibility in the application of oral history best practices. The outcome of this work, however, can offer insight into how the individual human heart and mind respond to the terror of an epidemic, and how an individual’s responses to fear and grief impact their communities.
The personal perspective oral history provides has so often been left out of our analysis of crisis. We are left with dry academic reports often composed by responding agencies trained to exclude emotion from their analysis. But without this emotion, without this individual perspective, we don’t understand crisis and the impact it has on those who are left to pick up the pieces of shattered lives and communities. Oral history provides a means for the people most affected by crisis or disaster to be recorded, archived, and shared, to put them, not the devastation, at the center of the story. It is an effort that often runs counter to our collective response to emergency and, for that reason alone, it offers meaningful and enduring outcomes.
Featured image: Hospital in Kenema, Sierra Leone, where the Ebola virus samples are tested. June 2014. By Leasmhar. CC-BY-SA-3.0 via Wikimedia Commons.
The reemergence of the Ebola epidemic provokes the kind of primal fear that has always gripped humans in the face of contagious disease, even though we now know more about how viruses work than ever before. Viruses, like all living organisms, are constantly evolving. This ensures that new viruses and their diseases will always be with us.
For thousands of years, people knew little about the “plagues” that afflicted them and, despite the impossibility to define causality, there were many attempts to explain how they happened.
Thucydides wrote in the History of the Peloponnesian War during the plague of Athens in 431 BCE that
“no pestilence of such extent nor any scourge so destructive of human lives is on record anywhere. For neither were physicians able to cope with the disease, since they at first had to treat it without knowing its nature, the mortality among them being greatest because they were most exposed to it, … And the supplications made at sanctuaries, or appeals to oracles and the like, were futile, and at last men desisted from them, overcome by the calamity.”
Even two thousand years later, scientists were at a loss to explain the workings of contagion. William Harvey, who described the circulation of blood in humans and is quoted in The Works of William Harvey by Tr. Robert Wills, wrote in 1653,
“So do I hold it scarcely less difficult to conceive how pestilence or leprosy should be communicated to a distance by contagion, by (an)…element contained in woolen or linen things, household furniture, even the walls of a house … How, I ask, can contagion, long lurking in such things … after a long lapse of time, produce its like nature in another body? Nor in one or two only, but in many, without respect of strength, sex, age, temperament, or mode of life, and with such violence that the evil can by no art be stayed or mitigated.”
In the absence of information, humankind resorted to any number of explanations for the origins of disease. Physicians, natural philosophers, and religious figures hypothesized causes of contagious diseases based on their view of the way the world worked. Disease theories became part of the discourse about the causes of events such as earthquakes, lightning and the movement of the planets.
Colorized transmission electron micrograph of Avian influenza A H5N1 viruses. virus. Centers for Disease Control and Prevention’s Public Health Image Library. Public domain via Wikimedia Commons.
Viruses are a fascinating group of entities that infect humans, other animals, plants, and bacteria. Their presence was anticipated when on 1 April 1717 Lady Mary Montagu, the wife of the British Ambassador to Turkey, wrote to a friend in England about smallpox. She was delighted to report that the disease did so little mischief. Why? Because an old woman would come with a “nutshell full of the matter of the best sort of small-pox,” (fluid derived from poxes) and immunize the children. The children would suffer some slight fever but soon recover, possibly never to contract the disease. What remained unknown was the contents of the fluid used by the old women to inoculate the children.
Near the close of the 19th century, scientists had come to understand that many plant diseases were caused by fungi, while a number of human diseases, such as tuberculosis, were caused by bacteria. But viruses remained a mystery.
That changed from the late 1880s to 1917, as the result of the discovery of contagious diseases whose causes could not be isolated or observed with ordinary microscopes. These included a contagion of tobacco plants, called mosaic disease, a disease of cattle (foot-and-mouth disease), yellow fever in humans, and another disease that attacked bacteria. It turned out they were all caused by viruses.
But the study of viruses posed unique challenges. Viruses are not cells like pathogenic bacteria or fungi which can multiply independently in their hosts or on artificial media. The agent that caused flu could not be grown in culture, and there was no experimental animal that could be infected. It was also impossible for researchers to visualize the agent of disease. After the great flu epidemic of 1918, scientists made numerous attempts to isolate the agent, but it was not until 1933 that three British investigators discovered that ferrets could be infected by nasal washings from patients with the disease. Thus they proved that an entity contained in nasal material could transmit the disease.
The mysteries of viruses were largely revealed by investigators working with those that infect bacteria. These viruses attracted the attention of researchers who speculated that they might lead to discoveries in the field of genetics. They worked with a virus that infects E. coli — which lives in the intestinal tracts of humans — and, while taking over the machinery of the bacterial cell, causes these bacteria to blow open, releasing hundreds of viral particles. Chemical analysis revealed their composition to be DNA and proteins. These studies contributed significantly to the conclusion that DNA is the genetic material of cellular life.
We now know that viruses that infect humans have their origin in animal populations that are in close contact with humans. Many of the flu viruses originate in Southeast Asia where bird and swine populations live in close proximity to humans. The viruses undergo mutations so that humans must be immunized each year against new strains. The rapid production of astronomical numbers of Ebola virus ensures that new strains will be constantly produced.
We also know that all viruses are composed of DNA or RNA and proteins. Ebola, influenza, polio, and AIDS are caused by RNA viruses. The virus that infects tobacco plants also is an RNA virus. Because we know how they work, we have had some success in interfering with the disease process with various drugs.
All of these modern procedures contribute to understanding the cause of disease. Humankind has long believed that understanding would lead to cures. As Hippocrates stated 2,500 years ago, “To know the cause of a disease and to understand the use of the various methods by which disease may be prevented amounts to the same thing in effect as being able to cure.”
And yet, as we have seen with Ebola, understanding the cause is not always the same as curing. We have arrived at a point in the 21st century where we can mitigate some contagious diseases and prevent other catastrophic diseases such as smallpox. But others will be with us now and in the future, for contagion is a general biological phenomenon, a natural phenomenon. Contagious agents evolve like all living organisms and constantly challenge us to understand their origin, spread and pathology.
Headline Image: Ebola virus. Centers for Disease Control and Prevention’s Public Health Image Library. Public domain via Wikimedia Commons.
In 1958, Henry Cabot Lodge Jr., the US ambassador to the United Nations, summarized the role of the world organization: “The primary, the fundamental, the essential purpose of the United Nations is to keep peace. Everything which does not further that goal, either directly or indirectly, is at best superfluous.” Some 30 years later another ambassador expressed a different view. “In the developing countries the United Nations… means environmental sanitation, agricultural production, telecommunications, the fight against illiteracy, the great struggle against poverty, ignorance and disease,” remarked Miguel Albornoz of Ecuador in 1985.
These two citations sum up the basic dilemma of the United Nations. It has always been burdened by high expectations: to keep peace, fix economic injustices, improve educational standards and combat various epidemics and pandemics. But inflated hopes have been tempered by harsh realities. There may not have been a World War III but neither has there been a day’s worth of peace on this quarrelsome globe since 1945. Despite all the efforts of the various UN Agencies (such as the United Nations Development Programme) and related organizations (like the World Bank), there exists a ‘bottom billion’ that survives on less than one dollar a day. The average lifespan in some countries barely exceeds thirty. According to UNESCO 774 million adults around the world lacked basic literacy skills in 2011.
Given such a seemingly dismal record, it is worth asking whether the UN has outlived its usefulness. After all, the organization turns 69 today (October 24th, 2014), a time when many citizens in the industrialized world exchange the stress of daily jobs for leisurely early retirement. Has the UN not had enough of a chance to keep peace and fix the world’s problems? Isn’t the obvious conclusion that the organization is a failure and the earlier it is scrapped the better?
The answer is no. The UN may not have made the world a perfect place but it has improved it immensely. The UN provides no definite guarantees of peace but it has been – and remains – instrumental for pacifying conflicts and enabling mediation between adversaries. Its humanitarian work is indispensable and saves lives every day. In simple terms: if the UN – or the various subsidiary organization that make up the UN – suddenly disappeared, lives would be lost and livelihoods would be endangered.
Henry Cabot, Jr. By Harris & Ewing. Public domain via Wikimedia Commons
In fact, the real question is not whether the UN has outlived its usefulness, but how can the UN perform better in addressing the many tasks it has been charged with?
The answer is twofold. First, the UN needs to be empowered to do what it does best. Today, for example, one of the most pressing global challenges is the potential spread of the Ebola virus. Driven by irrational fear, politicians in a number of countries suggest closing borders in order to safeguard their populations. But the only realistic way of addressing a virus that does not know national borders is surely international collaboration. In practical terms this means additional support for the World Health Organization (WHO), the only truly global organization equipped to deal with infectious diseases. But the WHO, much like the UN itself, is essentially a shoestring operation with a global mandate. Its budget in 2013 was just under 4 billion dollars. The US military spent that amount of money in two days.
Second, the UN must become better at ‘selling’ itself. Too much of what the UN and its specialized agencies do around the world is simply covered in fog. What about child survival and development (UNESCO)? Environmental protection (UNEP) and alleviation of poverty (UNDP)? Peaceful uses of atomic energy (IAEA)? Why do we hear so little about the UN’s (or the International Labour Organization’s) role in improving workers’ rights? Does anyone know that the UNHCR has been awarded the Nobel Peace Prize twice (out of a total of 11 Nobel Peace Prizes awarded to the UN, its specialized agencies, related agencies, and staff)? It’s not a bad CV!
We tend to hear, ad nauseam, that the 21st century is a globalized one, filled with global problems but apparently lacking in global solutions. What we tend to forget is the simple fact that there exists an organization that has been addressing such global challenges – with limited resources and without fanfare – for almost seven decades.
Indeed, it seems that in today’s world the UN is more relevant than ever before. At 69 it is certainly not ripe for retirement.
Featured image credit: United Nations Flags, by Tom Page. CC-BY-SA-2.0 via Wikimedia Commons
The outbreak of Ebola, in Africa and in the United States, is a stark reminder of the clear and present danger that infection represents in all our lives, and we need reminding. Despite all of our medical advances, more familiar infections still take tens of thousands of American lives each year – and too often these deaths are avoidable.
Hospital infections kill 75,000 Americans a year — more than twice the number of people who die in car crashes. Most people know that motor vehicle deaths could be drastically reduced. What’s not as widely appreciated is that the far greater number of hospital infections could be reduced by up to 70%.
Changes that would reduce infections are evidence-based and scientific, supported by the Centers for Disease Control and Prevention. For example, the campaign against hospital-acquired urinary tract infection — one of the most common hospital infections in the world — seeks to minimize the use of internal, Foley catheters, a major vector of infection. Nurses who have always relied on Foleys to deal with patients who have urinary incontinence are told to use straight catheters intermittently instead, which increases their workload. Surgeons who are accustomed to placing Foley catheters in their patients for several days after an operation are told to remove the catheter shortly after surgery – or not to use one at all. Similar approaches can be used to reduce other common infections. If we know what needs to be done to lower the rate of hospital infections, why have the many attempts to do so fallen so woefully short?
Our research shows that a major reason is the unwillingness of some nurses and physicians to support the desired new behaviors. We have found that opposition to hospitals’ infection prevention initiatives comes from the three groups we call Active Resisters, Organizational Constipators, and Timeservers. While we know these types of individuals exist in hospitals since we have seen them in action, we suspect they can also be found in all types of organizations.
Active resisters refuse to abide by and sometimes campaign against an initiative’s proposed changes. Some active resisters refuse to change a practice they have used for years because they fear it might have a negative impact on their patients’ health. Others resist because they doubt the scientific validity of a change, or because the change is inconvenient. For others it’s simply a matter of ego, as in, “Don’t tell me what to do.” Some ignore the evidence. Many initiatives to prevent urinary tract infection ask nurses to remind physicians when it’s time to remove an indwelling catheter, but many nurses are unwilling to confront physicians – and many physicians are unwilling to be so confronted.
Organizational constipators present a different set of challenges. Most are mid- to upper-level staff members who have nothing against an infection prevention initiative per se but simply enjoy exercising their power. Sometimes they refuse to permit underlings to help with an initiative. Sometimes they simply do nothing, allowing memos and emails to pile up without taking action. While we have met some physicians in this category, we have seen, unfortunately, a surprising number of nursing leaders employ this approach.
Timeservers do the least possible in any circumstance. That applies to every aspect of their work, including preventing infection. A timeserver surgeon may neglect to wash her hands before examining a patient, not because she opposes that key infection prevention requirement but because it’s just easier that way. A timeserver nurse may “forget” to conduct “sedation vacations” for patients who are on mechanical breathing machines to assess if the patient can be weaned from the ventilator sooner for the simple reason that sedated patients are less work.
We have learned that different overcoming these human-related barriers to improvement requires different styles of engagement.
To win support among the active resisters, we recommend employing data both liberally and strategically. Doctors are trained to respond to facts, and a graph that shows a high rate of infection department can help sway them. Sharing research from respected journals describing proven methods of preventing infection can also help overcome concerns. Nurse resisters are similarly impressed by such data, but we find that they are also likely to be convinced by appeals to their concern for their patients’ welfare – a description, for example, of the discomfort the Foley causes their patients.
Organizational constipators and timeservers are more difficult to win over, largely because their negative behavior is an incidental result of their normal operating style. Managers sometimes try to work around the organizational constipators and assign an authority figure to harass the timeservers, but their success is limited. Efforts to fire them can sometimes be difficult.
Hospitals’ administrative and medical leaders often play an important role in successful infection prevention initiatives by emphasizing their approval in their staff encounters, by occasionally attending an infection prevention planning session, and by making adherence to the goals of the initiative a factor in employee performance reviews. Some innovative leaders also give out physician or nurse champion-of-the-year awards that serve the dual purpose of rewarding the healthcare workers who have been helpful in a successful initiative while encouraging others by showing that they, too, could someday receive similar recognition. It may help to include potential obstructors in planning for an infection prevention campaign; the critics help spot weaknesses and are also inclined to go easy on the campaign once it gets underway.
But the leadership of a successful infection prevention project can also come from lower down in a hospital’s hierarchy, with or without the active support of the senior executives. We found the key to a positive result is a culture of excellence, when the hospital staff is fully devoted to patient-centered, high-quality care. Healthcare workers in such hospitals endeavor to treat each patient as a family member. In such institutions, a dedicated nurse can ignite an infection prevention initiative, and the staff’s all-but-universal commitment to patient safety can win over even the timeservers. The closer the nation’s hospitals approach that state of grace, the greater the success they will have in their efforts to lower infection rates.
Preventing infection is a team sport. Cooperation — among doctors, nurses, microbiologists, public health officials, patients, and families — will be required to control the spread of Ebola. Such cooperation is required to prevent more mundane infections as well.
When the UN General Assembly endorsed the Responsibility to Protect (R2P) in 2005, the members of the United Nations recognized the responsibility of states to protect the basic human and humanitarian rights of the world’s citizens. In fact, R2P articulates concentric circles of responsibility, starting with the individual state’s obligation to ensure the well-being of its own people; nested within the collective responsibility of the community of nations to assist individual states in meeting those obligations; in turn encircled by the responsibility of the United Nations to respond if necessary to ensure the basic rights of civilians, with military means only contemplated as a last resort, and only with the consent of the Security Council.
The Responsibility to Protect is a response to war crimes, genocide, and other crimes against humanity. But R2P is also a response to pattern and practice human rights abuses that include entrenched poverty, widespread hunger and malnutrition, and endemic disease and denials of basic health care — all socio-economic conditions which themselves feed and exacerbate armed conflict. In fact, socio-economic development is a powerful mechanism for guaranteeing the full panoply of human rights, just as the Millennium Development Goals are a means of fulfilling the Responsibility to Protect.
While Responsibility to Protect is often misconstrued as a mandate for military action, it is more intrinsically a call to social action, and the embodiment of the joint and several responsibilities of the community of nations to seek a coordinated global response to life-threatening conditions of armed conflict, repression, and socio-economic misery. While diplomats and public servants debate the legality and prudence of military responses to criminal uses of military force against civilians, we must not neglect the legality, prudence, and urgency of non-military responses to public health and poverty emergencies throughout the world.
The United States has put out a call to like-minded nations to join forces, literally and figuratively, in the degradation and destruction of the criminal militancy of the so-called Islamic State [ISIL or ISIL]. Despite concerns that the 2003-2011 US war in Iraq itself may have led to the inception and flourishing of ISIS, and despite warnings that the training, arming, and assisting of Iraqi forces, Shia militias in Iraq and non-ISIS Sunni militants in Syria may inflame sectarian violence and threaten civilians in both countries, the United States is contemplating another open-ended military intervention in the Levant.
A military intervention against ISIS is not justified by the principles of Responsibility to Protect. Without the authorization of the Security Council or the consent of the Syrian government, military intervention is unlawful in Syria, offending both the UN Charter and the tenets of R2P. In either Syria or Iraq a military intervention, even with the permission of the responsible governments, is unlawful if it is likely to lead to further outrages against civilians. Military action that predictably causes the suffering of civilians disproportionate to any legitimate military objectives violates the principles of humanitarian law and the Geneva Conventions, as well as the UN Charter and R2P.
UNICEF and partners visit the crowded Marché Niger to continue explaining to families how to they can protect themselves from Ebola. UNICEF have visited many markets, churches, mosques, schools, and community centers throughout Conakry and in the Forest region where the outbreak began. CC BY-NC 2.0 via UNICEF Guinea Flickr.
Alongside the criminal militancy of ISIS we face the existential threat of the Ebola virus in West Africa, endangering the people of Guinea, Liberia, Sierra Leone, and their neighbors. Over the past two months, approximately 5000 people have been infected by this hemorrhagic disease, and around 2500 have died, over 150 of them health care workers. At current rates of infection, with new cases doubling every three weeks, the virus could sicken 10,000 by the end of September, 40,000 by mid-November, and 120,000 by the New Year.
Ebola can be contained through basic public health responses: quarantining of the sick, tracing of exposure in families and communities, safe recovery of the bodies of the deceased, regular hand-washing and sanitation, and the all-important rebuilding of trust between effected community members, health care workers, and government officials. But the very countries impacted have fragile health care systems, insufficient hospital beds, and dedicated Red Cross workers, doctors, and nurses nearly besieged by the number of sick people needing care. By funding and supporting more health care and humanitarian relief workers at the international and local levels, more Ebola field hospitals and clinics, and more food, rehydration fluids, and safe blood supplies for transfusions, less new people will fall sick, and more of the infected will be treated and cured. At the same time, the fragile economies and political systems of the effected countries will be strengthened and the threat of regional insecurity will be addressed. Ebola in West Africa is calling out for a coordinated global public health intervention, which will serve our Responsibility to Protect at the local level, while furthering our collective security at the global level.
As the US Congress debates the funding of so-called moderate rebels in Syria in the pursuit of containing the criminal militancy of ISIS, we should turn our national attention to funding Ebola emergency relief in Guinea, Liberia, and Sierra Leone. Such action is consistent with our enlightened self-interest, and required by our humanitarian principles and obligations.
Ebola is a widely known, but poorly understood, virus. Even in West Africa, in the middle of the 2014 West African Ebola Epidemic, the vast majority of patients with a differential diagnosis of Ebola Virus Disease (EVD) will in fact be suffering with something else serious and potentially fatal. The possibility of EVD should not over-shadow other investigations and management.
Peter Piot’s team discovered Ebola in 1976 – he’s now the head of the London School of Tropical Medicine and was reassuringly quoted in 2014 as saying ‘I would sit next to an infected person on a train’. It is one of two Filoviruses (the other being Marburg) and according to the CDC, it has caused thirty-four outbreaks, twenty-four of which have been in Sub-Saharan Africa, with total fatalities numbering only in the thousands. Transmission relies on direct contact with bodily fluids containing the virus, either through broken-skin or through mucous membranes. Airborne, droplet- aerosol transmission does not seem to be a popular mechanism of spread, though it is possible that this does occur. Symptoms are visible as soon as people are contagious and Ebola Virus is not, therefore, what Piot termed the ‘right kind of virus’ to start an epidemic in a major western city. It is conceivable that an outbreak could occur, but it lends itself to active case finding, contact tracing, and containment far more easily than, for example, the flu-viruses.
Ebola Virus Particles: Colorized scanning electron micrograph of filamentous Ebola virus particles (green) attached to and budding from a chronically infected VERO E6 cell (blue) (25,000x magnification). Credit: NIAID. CC BY 2.0 via NIAID Flickr.
Its relative fame therefore, is probably related to three aspects of EVD: the extremely high (both untreated and treated) case fatality rates (as high as 90% in some outbreaks); the extremely rapid onset and dramatic nature of its symptoms (it is a hemorrhagic fever and death is usually preceded by haemorrhage and widespread organ necrosis); and finally the enigmatic nature of the outbreaks–the animal reservoir is not yet clarified (though fruit bats are currently the most likely candidate). This last aspect allows popular descriptions of the virus to describe it as lurking in the sinister darkness of the African jungle, waiting to emerge on an unsuspecting population.
If you work in the global north in a modern, well-equipped hospital, the management of a low-risk of an extremely dangerous event must be governed by national and international protocols rather than the arbitrary decisions of individual clinicians. Members of medical teams should ensure that these protocols are available, and followed – they govern isolation techniques, blood sample procurement and delivery, and contact tracing.
If you work in a region where Ebola epidemics are a possibility then you will be faced with a vast number of challenges to identify and manage these cases: poor data collection and management systems, weak public health infrastructure, limited availability of personal protective equipment and, perhaps most importantly, a population who are vulnerable because of (in many cases) limited education, weakened immunity and cultural practices that encourage transmission. In these contexts the epidemic potential of the virus is greatly magnified. The 2014 epidemic has demonstrated that the international community is quite content to allow widespread transmission across several countries until expatriates are affected. The overstretched expatriate and national staff of the responding agencies have two jobs – to manage as best they can with epidemic control and to advocate for, and demand the vast resources – human and financial – that are needed to control the spread of a disease that reflects poverty and lack of long term investment in regions of the world that are vulnerable to so many other threats to life and health.
Until the current epidemic, Ebola was largely regarded as not a Western problem. Although fearsome, Ebola seemed contained to remote corners of Africa, far from major international airports. We are now learning the hard way that Ebola is not—and indeed was never—just someone else’s problem. Yes, this outbreak is different: it originated in West Africa, at the border of three countries, where the transportation infrastructure was better developed, and was well under way before it was recognized. But we should have understood that we are “all in this together” for Ebola, as for any, infectious disease.
Understanding that we were profoundly wrong about Ebola can help us to see ethical considerations that should shape how we go forward. Here, I have space just to outline two: reciprocity and fairness.
In the aftermath of the global SARS epidemic that spread to Canada, the Joint Centre for Bioethics at the University of Toronto produced a touchstone document for pandemic planning, Stand on Guard for Thee, which highlights reciprocity as a value. When health care workers take risks to protect us all, we owe them special concern if they are harmed. Dr. Bruce Ribner, speaking on ABC, described Emory University Hospital as willing to take two US health care workers who became infected abroad because they believed these workers deserved the best available treatment for the risks they took for humanitarian ends. Calls to ban the return of US workers—or treatment in the United States of other infected front-line workers—forget that contagious diseases do not occur in a vacuum. Even Ann Coulter recognized, in her own unwitting way, that we owe support to first responders for the burdens they undertake for us all when she excoriated Dr. Kent Brantly for humanitarian work abroad rather than in the United States.
We too often fail to recognize that all the health care and public health workers at risk in the Ebola epidemic—and many have died—are owed duties of special concern. Yet unlike health care workers at Emory, health care workers on the front lines in Africa must make do with limited equipment under circumstances in which it is very difficult for them to be safe, according to a recent Wall Street Journal article. As we go forward we must remember the importance of providing adequately for these workers and for workers in the next predictable epidemics — not just for Americans who are able to return to the US for care. Supporting these workers means providing immediate care for those who fall ill, as well as ongoing care for them and their families if they die or are not longer able to work. But this is not all; health care workers on the front lines can be supported by efforts to minimize disease spread—for example conducting burials to minimize risks of infection from the dead—as well as unceasing attention to the development of public health infrastructures so that risks can be swiftly identified and contained and care can be delivered as safely as possible.
Fairness requires treating others as we would like to be treated ourselves. A way of thinking about what is fair is to ask what we would want done if we did not know our position under the circumstances at hand. In a classic of political philosophy, A Theory of Justice, John Rawls suggested the thought experiment of asking what principles of justice we would be willing to accept for a society in which we were to live, if we didn’t know anything about ourselves except that we would be somewhere in that society. Infectious disease confronts us all with an actual possibility of the Rawlsian thought experiment. We are all enmeshed in a web of infectious organisms, potential vectors to one another and hence potential victims, too. We never know at any given point in time whether we will be victim, vector, or both. It’s as though we were all on a giant airplane, not knowing who might cough, or spit, or bleed, what to whom, and when. So we need to ask what would be fair under these brute facts of human interconnectedness.
At a minimum, we need to ask what would be fair about the allocation of Ebola treatments, both before and if they become validated and more widely available. Ethical issues such as informed consent and exploitation of vulnerable populations in testing of experimental medicines certainly matter but should not obscure that fairness does, too, whether we view the medications as experimental or last-ditch treatment. Should limited supplies be administered to the worst off? Are these the sickest, most impoverished, or those subjected to the greatest risks, especially risks of injustice? Or, should limited supplies be directed where they might do the most good—where health care workers are deeply fearful and abandoning patients, or where we need to encourage people who have been exposed to be monitored and isolated if needed?
These questions of fairness occur in the broader context of medicine development and distribution. ZMAPP (the experimental monoclonal antibody administered on a compassionate use basis to the two Americans) was jointly developed by the US government, the Public Health Agency of Canada, and a few very small companies. Ebola has not drawn a great deal of drug development attention; indeed, infectious diseases more generally have not drawn their fair share of attention from Big Pharma, as least as measured by the global burden of disease.
WHO has declared the Ebola epidemic an international emergency and is convening ethics experts to consider such questions as whether and how the experimental treatment administered to the two Americans should be made available to others. I expect that the values of reciprocity and fairness will surface in these discussions. Let us hope they do, and that their import is remembered beyond the immediate emergency.
Headline Image credit: Ebola virus virion. Created by CDC microbiologist Cynthia Goldsmith, this colorized transmission electron micrograph (TEM) revealed some of the ultrastructural morphology displayed by an Ebola virus virion. Centers for Disease Control and Prevention’s Public Health Image Library, #10816 . Public domain via Wikimedia Commons.
The Ebola outbreak affecting Guinea, Sierra Leone, Nigeria and now Liberia is the worst since this disease was first discovered more than 30 years back. Between 1976 and 2013 there were less than 1,000 known infections. According to the Centers for Disease Control and prevention (CDC), March to 23 July 2014 saw 1201 likely cases and 672 deaths. The ongoing situation for these four West African countries is extremely dangerous, and there are fears that it could spread more widely in Africa. The relatively few intensive care units are being overwhelmed and the infection rate is likely being exacerbated by the fact that some who become ill are, on hearing that there is no specific treatment, electing to die at home surrounded by their family. The big danger is that very sick patients bleed, and body fluids and blood are extremely infectious.
American Patrick Sawyer, who was caring for his ill sister in Nigeria, has died of the disease. Working with the Christian AID Agency Samaritan’s Pulse in Monrovia, Dr Kent Brantly from Texas and Nancy Writebol from North Carolina are thought to have been infected following contact with a local staff member. Both are symptomatic but stable as I write this (July 31).
Ebola cases are classically handled by isolation, providing basic fluid support, and “barrier nursing”. Ideally, that means doctors and nurses wear disposable gowns, quality facemasks, eye protection and (double) latex gloves. That’s why it is so dangerous for patients to be cared for at home. And, even when professionals are involved, the highest incidence of infection is normally in health care workers. A number of doctors have died in the current outbreak. If there’s any suspicion that travelers returning from Africa may be infected, it is a relatively straightforward matter in wealthy, well-organized countries like the USA to institute appropriate isolation, nursing, and control. That’s why the CDC believes that the threat to North America is minimal. As for so many issues, the problem in Africa is exacerbated by poverty and the social disruption that goes with a lack of basic resources.
Given that this disease is not a constant problem for humans, where does it hide out? Fruit bats are thought to be the natural and asymptomatic reservoir, though, unlike the hideous and completely unrelated Hendra and Nipah viruses that have caused somewhat similar symptoms in Australia and South East Asia, there is no Ebola virus in bats from those regions. And, while Hendra and Nipah are lethal for horses and pigs respectively, Ebola is killing off the great apes including our close and endangered primate relatives, the Chimpanzees and Gorillas. The few human Hendra infections have been contracted from sick horses that were, in turn, infected from fruit bats. An “index” (first contact) human Ebola case could result from exposure to bat droppings, or from killing wild primates for “bush meat” a practice that is, again, exacerbated by poverty. And, unlike Hendra, Ebola is known to spread from person to person.
The early Ebola symptoms of nausea, fever, headaches, vomiting, diarrhea, and general malaise are not that different from those characteristic of a number of virus infections, including severe influenza. But Ebola progresses to cause the breakdown of blood vessel walls and extensive bleeding. Also, unlike the fast developing influenza, the Ebola incubation period can be as long as two to three weeks, which means that there must be a relatively long quarantine period for suspected contacts. Fortunately, and unlike influenza and the hideous (fictional) bat-origin pathogen depicted in the recent movie Contagion, Ebola is, in the absence of exposure to contaminated body fluids, not all that infectious. Unlike most such Hollywood accounts, Contagion is relatively realistic and describes how government public health laboratories like the CDC operate. It’s worth seeing, and has been described as “the thinking person’s horror movie.”
Along with comparable EEC agencies and the WHO, the CDC currently has about 20 people “on the ground” in West Africa. Other support is being provided by organizations like Doctors Without Borders, the International Red Cross, and so forth. At this stage, there are no antiviral drugs available and no vaccine, though there are active research programs in several institutions, including the US NIH Vaccine Research Center in Bethesda, Maryland. Though there is no product currently available, it would be a big plus if all African healthcare workers could be vaccinated against Ebola. Apart from develop specific “small molecule” drugs, monoclonal antibodies (mAbs) that bind to proteins on the surface of the virus may be useful for emergency treatment and to give those in contact “passive” protection for three or four weeks. Such “miraculous mAbs” can now be developed and produced quickly, though they are very expensive.
What is being done? Neighboring African countries are closing their borders. International agencies and governments are providing more professionals and other resources to help with treatment and tracking cases and contacts. Global companies have been withdrawing their workers and all nations are maintaining a close watch on air travelers who are arriving from, or have recently been in, these afflicted nations.
What is this Ebola catastrophe telling us? In these days of global cost-cutting, we must keep our National and State Public Health Services strong and maintain the funding for UN Agencies like the OIE, the WHO, and the FAO. High security laboratories (BSL4) at the CDC, the NIH and so forth are a global resource, and their continued support along with the training and resourcing of the courageous, dedicated physicians and researchers who work with these very dangerous pathogens, is essential. Humanity is constantly challenged by novel, zoonotic viruses like Ebola, Hendra, Nipah, Sin Nombre, SARS, and MERS that emerge out of wildlife reservoirs, with the likelihood of such events being increased by extensive forest clearing, ever increasing population size and rapid air travel. We must be indefatigably watchful and prepared. Throughout history, nature is our worst bioterrorist.
Peter C. Doherty has appointments at the University of Melbourne, Australia, and St Jude Children’s Research Hospital, Memphis. He is the 2013 author of Pandemics: What Everyone Needs to Know, which looks at the world of pandemic viruses and explains how infections, vaccines and monoclonal antibodies work . He shared the 1996 Nobel Prize for Physisology or Medicine for his discoveries concerning “The Cellular Immune Defense”.
What Everyone Needs to Know (WENTK) series offers a balanced and authoritative primer on complex current event issues and countries. Written by leading authorities in their given fields, in a concise question-and-answer format, inquiring minds soon learn essential knowledge to engage with the issues that matter today.
Subscribe to the OUPblog via email or RSS.
Subscribe to only health and medicine articles on the OUPblog via email or RSS.
With the Ebola virus in the news recently, you may be wondering what actions you can take to reduce the risk of contracting and spreading the deadly disease. Expert Peter C. Doherty provides valuable pointers on the best ways to stay safe and healthy in this excerpt from Pandemics: What Everyone Needs to Know answering: Is there anything that I can do personally to limit the possibility of a dangerous pandemic?
While pandemics are by their nature unpredictable, there are some things worth considering when it comes to the issue of personal safety and responsibility. The first point is to be a safe international traveler so that you don’t bring some nasty infection home with you. Protect yourself and you protect others. Though taking the available vaccines won’t prevent infection with some novel pathogen, it will contribute toward ensuring that you enjoy a successful vacation or business trip, and it should also put you in a “think bugs” mind-set. If, for instance, you are off to Africa for a wildlife safari, make an appointment at a travel clinic (or with your primary care physician) two to three months ahead of time to check your vaccine status and, if needed, receive booster shots to ensure that your antibody levels are high. Anyone who is visiting a developing country should make sure that he or she has indeed received the standard immunizations of childhood. Adolescents and young adults are much more likely to suffer severe consequences if, for instance, they contract commonplace infections like measles or mumps that have, because of herd immunity, become so unusual in Western countries that a minority of parents reject the collective responsibility of vaccinating their kids. If you’re younger and your parents are (or were) into alternative lifestyles, it may be wise to ask them very directly about your personal immunization history.
It’s also likely that, even if you were vaccinated early on, your level of immunity will have declined greatly and you will benefit from further challenge. Both possibilities will be covered if you go to a comprehensive travel clinic, as the doctors and nurses there will insist that you receive these shots (or a booster) if you don’t have a documented recent history. Any vaccination schedule should ideally be completed at least 3 to 4 weeks ahead of boarding your flight, the time needed for the full development of immunity. But this is one situation where “better late than never” applies. Should it have slipped your mind until the last minute, you should be vaccinated nevertheless. Even if you’ve never had that particular vaccine before, some level of protection could be there within 5 to 10 days, and a boosted, existing response will cut in more quickly. A travel clinic will also sell you a Gastro (gastroenteritis, not gastronomy) kit containing antibiotics to counter traveler’s diarrhea (generally a result of low-grade E. coli infection), something to decrease intestinal/gastric motility (Imodium), and sachets of salts to restore an appropriate fluid balance.
For the elderly, be aware of the decline in immunity that happens with age. You may not respond to vaccines as well as those who are younger, and you will be at greater risk from any novel infection. Depending on your proposed itinerary, it may also be essential to take anti-malarial drugs, which generally have to be started well ahead of arrival. Malaria is not the only mosquito-borne threat in tropical countries, so carry a good supply of insect repellant. In general, think about when and where you travel. Avoiding the hot, wet season in the tropics may be a good idea, both from the aspect that too much rain can limit access to interesting sites and because more standing water means more mosquitoes. Wearing long trousers, long-sleeved shirts, and shoes and socks helps to protect against being bitten (both by insects and by snakes), while also minimizing skin damage due to higher UV levels. Then, before you make your plans and again prior to embarking, check the relevant websites at the CDC, the WHO, and your own Department of Foreign Affairs (Department of State in the United States) for travel alerts. Especially if they’re off to Asia, many of my medical infectious disease colleagues travel with one or other of the antiviral drugs (Relenza and Tamiflu) that work against all known influenza strains. These require a prescription, but they’re worth having at home anyway in case there is a flu pandemic. If that happens, the word will be out that influenza is raging and stocks in the pharmacies and drugstores will disappear very quickly. But don’t rely on self-diagnosis if you took your Tamiflu with you to some exotic place; see a doctor. What you may think is flu could be malaria.
For those who may be sexually active with a previously unknown partner, carry prophylactics (condoms) and behave as responsibly as possible. Excess alcohol intake increases the likelihood that we will do something stupid. Dirty needles must be avoided, but don’t inject drugs under any circumstances. Blood-borne infections with persistently circulating viruses (HIV and hepatitis B and C) are major risks, while insect-transmitted pathogens (dengue, Chikungunya, Japanese B encephalitis) can also be in the human circulation for 5–10 days. Apart from that, being caught with illegal drugs can land you in terrible trouble, particularly in some Southeast Asian nations. No matter what passport you carry, you are subject to the laws of the country. Be aware that rabies may be endemic and that animal bites in general can be dangerous.
Can you really trust a tattooist to use sterile needles? Even if the needles are clean, what about the inks? How can they be sterilized to ensure that they are not, as has been known to occur, contaminated with Mycobacterium chelonae, the cause of a nasty skin infection? And that was in the United States, not in some exotic location where there may be much nastier bugs around.
Peter C. Doherty is Chairman of the Department of Immunology at St. Jude’s Children’s Research Hospital, and a Laureate Professor of Microbiology and Immunology at the University of Melbourne. He is the author of Pandemics: What Everyone Needs to Know, The Beginner’s Guide to Winning the Nobel Prize: Advice for Young Scientists, Their Fate is Our Fate: How Birds Foretell Threats to Our Health and Our World, and A Light History of Hot Air.
What Everyone Needs to Know (WENTK) series offers a balanced and authoritative primer on complex current event issues and countries. Written by leading authorities in their given fields, in a concise question-and-answer format, inquiring minds soon learn essential knowledge to engage with the issues that matter today. Starting July 2014, OUPblog will publish a WENTK blog post monthly.
Subscribe to the OUPblog via email or RSS.
Subscribe to only health and medicine articles on the OUPblog via email or RSS.
Image credit: Ebola virus particles by Thomas W. Geisbert, Boston University School of Medicine. Public Domain via Wikimedia Commons.
A recent New York Times editorial by author David Quammen highlighted the seriousness of the current Ebola outbreak in Guinea, but made the point that there is no great risk of any global pandemic. That’s been generally true of the viruses that, like Ebola, cause exudative diathesis, or bleeding into the tissues, and present with horrific symptoms. There’s a whole range of such infections caused by a spectrum of different virus types. These pathogens are generally maintained asymptomatically in wildlife “reservoir” species, including fruit and insectivorous bats, monkeys, field mice, and various other rodent species. Breathing dust contaminated with dried mouse feces can lead, for example, to infection with the Sin Nombre hantavirus that caused a recent outbreak in Yellowstone National Park. Others (like Ebola) may “jump” across to us from bats and are then transmitted between people following contact with contaminated human blood and other secretions.
Ebola virus virion.
From the pandemic aspect, the most dangerous we’ve seen to date is the SARS coronavirus that, in 2002, came out of nowhere to kill some 800 people in the Asia/Pacific region and also caused cases in Toronto. Spread via the respiratory route or by hand-to-face transmission following contact with contaminated surfaces this virus would, if it had emerged prior to the 19th century development of the germ theory of infectious disease, have gone on to cause a continuing human problem. As it was, once the virologists had identified the virus and worked out its mechanism of spread, instituting rigorous sanitation procedures (especially hand washing) and practicing “barrier nursing” (latex gloves, face masks, disposable gowns) with afflicted patients led to the disease essentially “burning out” in humans. Authorities in the Middle East are, though, keeping a close watch on the closely related MERS coronavirus, which has caused a few human cases and may be maintained in nature as an asymptomatic infection of Egyptian tomb bats and camels. Could the MERS-CoV be the source of “The Curse of the Mummy’s Tomb”?
Even in the absence of specific antiviral drugs and vaccines, modern science protects us by defining the problem so that public health and medical professionals can take appropriate counter-measures. Still, though such viruses do not generally change their mode of transmission to spread readily by the dangerous respiratory route (we can’t choose when and where to breathe!), the basic message is that the price of freedom (from such infections) is constant vigilance. That’s why government agencies like the CDC and the US Public Health Service are so important for our defense. So far, the “worst-case” pandemic scenario for any hemorrhagic fever virus is that portrayed in the movie Contagion. Hopefully, a catastrophe of such magnitude will remain in the realm of fiction, but we do need to keep our guard up. The much more immediate and likely pandemic danger is always, so far as we are aware, from the influenza A viruses.
Peter C. Doherty is Chairman of the Department of Immunology at St. Jude’s Children’s Research Hospital, and a Laureate Professor of Microbiology and Immunology at the University of Melbourne. He is the author of The Beginner’s Guide to Winning the Nobel Prize: Advice for Young Scientists, Their Fate is Our Fate: How Birds Foretell Threats to Our Health and Our World, published in Australia as Sentinel Chickens: What Birds Tell us About Our health and the World,A Light History of Hot Air and Pandemics: What Everyone Needs to Know.
Subscribe to the OUPblog via email or RSS.
Subscribe to only science and medicine articles on the OUPblog via email or RSS.









 “The love of my life and the father of my son came to America to marry me. It was supposed to be the first happy day of a new life of joy for us all. But before we could make our new family, he died a terrible death in a quarantined room… I am writing this book to tell people about Eric, about our love story, about our family, and about my faith that has been tested but not broken.”
“The love of my life and the father of my son came to America to marry me. It was supposed to be the first happy day of a new life of joy for us all. But before we could make our new family, he died a terrible death in a quarantined room… I am writing this book to tell people about Eric, about our love story, about our family, and about my faith that has been tested but not broken.”

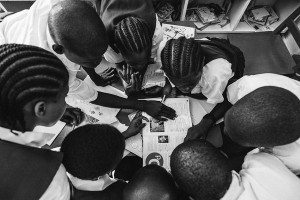








![Dr. Joel Montgomery, Team Lead for CDC’s Ebola Response Team in Liberia, adjusts a colleague’s [personal protective equipment] before entering the Ebola treatment unit. Photograph by Athalia Christie. Public domain via Flickr.](http://blogoup.electricstudiolt.netdna-cdn.com/wp-content/uploads/2014/10/Mark-Cave-Ebola-Crisis-2-e1414089239337.jpg)




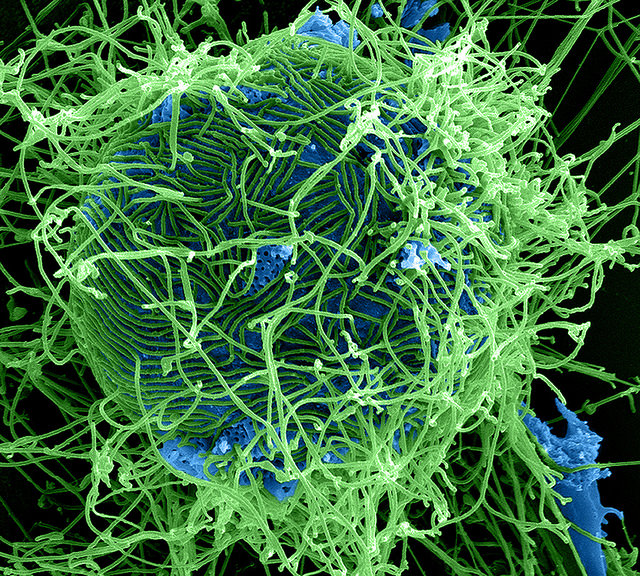




Amen!!!! Very well said!!! *applause*
Reblogged this on Jo Robinson.
Please tell Meredith she writes right. And thank you for being such a lovely dad.
Bravo. Very well said from a girl with a big heart. As long as it doesn’t effect us it’s not very real. Thanks for posting this Mark.
Excellent points from your daughter who has inherited the very best of her mother So glad you posted this, Jo!