First isolated in Uganda in 1947, this normally mild, non-fatal mosquito-born flavivirus infection is characterized by transient fever, joint pain and malaise. The current explosive Zika virus epidemic in the Americas is, however, causing great concern because of what looks to be a sudden, dramatic increase in the incidence of microcephaly (small brain/head size) in newborns.
The post The Zika virus: a “virgin soil” epidemic appeared first on OUPblog.

By Peter C. Doherty
The Ebola outbreak affecting Guinea, Sierra Leone, Nigeria and now Liberia is the worst since this disease was first discovered more than 30 years back. Between 1976 and 2013 there were less than 1,000 known infections. According to the Centers for Disease Control and prevention (CDC), March to 23 July 2014 saw 1201 likely cases and 672 deaths. The ongoing situation for these four West African countries is extremely dangerous, and there are fears that it could spread more widely in Africa. The relatively few intensive care units are being overwhelmed and the infection rate is likely being exacerbated by the fact that some who become ill are, on hearing that there is no specific treatment, electing to die at home surrounded by their family. The big danger is that very sick patients bleed, and body fluids and blood are extremely infectious.
American Patrick Sawyer, who was caring for his ill sister in Nigeria, has died of the disease. Working with the Christian AID Agency Samaritan’s Pulse in Monrovia, Dr Kent Brantly from Texas and Nancy Writebol from North Carolina are thought to have been infected following contact with a local staff member. Both are symptomatic but stable as I write this (July 31).
Ebola cases are classically handled by isolation, providing basic fluid support, and “barrier nursing”. Ideally, that means doctors and nurses wear disposable gowns, quality facemasks, eye protection and (double) latex gloves. That’s why it is so dangerous for patients to be cared for at home. And, even when professionals are involved, the highest incidence of infection is normally in health care workers. A number of doctors have died in the current outbreak. If there’s any suspicion that travelers returning from Africa may be infected, it is a relatively straightforward matter in wealthy, well-organized countries like the USA to institute appropriate isolation, nursing, and control. That’s why the CDC believes that the threat to North America is minimal. As for so many issues, the problem in Africa is exacerbated by poverty and the social disruption that goes with a lack of basic resources.

The fight against Ebola in West Africa… 4 months after the first case of Ebola was confirmed in Guinea, more than 1200 people have been infected across 3 West African countries. This biggest Ebola outbreak ever recorded requires an intensification of efforts to avoid it from spreading further and claiming many more lives. Photo credits: ©EC/ECHO/Jean-Louis Mosser. EU Humanitarian Aid and Civil Protection. CC BY-ND 2.0 via European Commission DG ECHO Flickr.
Given that this disease is not a constant problem for humans, where does it hide out? Fruit bats are thought to be the natural and asymptomatic reservoir, though, unlike the hideous and completely unrelated Hendra and Nipah viruses that have caused somewhat similar symptoms in Australia and South East Asia, there is no Ebola virus in bats from those regions. And, while Hendra and Nipah are lethal for horses and pigs respectively, Ebola is killing off the great apes including our close and endangered primate relatives, the Chimpanzees and Gorillas. The few human Hendra infections have been contracted from sick horses that were, in turn, infected from fruit bats. An “index” (first contact) human Ebola case could result from exposure to bat droppings, or from killing wild primates for “bush meat” a practice that is, again, exacerbated by poverty. And, unlike Hendra, Ebola is known to spread from person to person.
The early Ebola symptoms of nausea, fever, headaches, vomiting, diarrhea, and general malaise are not that different from those characteristic of a number of virus infections, including severe influenza. But Ebola progresses to cause the breakdown of blood vessel walls and extensive bleeding. Also, unlike the fast developing influenza, the Ebola incubation period can be as long as two to three weeks, which means that there must be a relatively long quarantine period for suspected contacts. Fortunately, and unlike influenza and the hideous (fictional) bat-origin pathogen depicted in the recent movie Contagion, Ebola is, in the absence of exposure to contaminated body fluids, not all that infectious. Unlike most such Hollywood accounts, Contagion is relatively realistic and describes how government public health laboratories like the CDC operate. It’s worth seeing, and has been described as “the thinking person’s horror movie.”
Along with comparable EEC agencies and the WHO, the CDC currently has about 20 people “on the ground” in West Africa. Other support is being provided by organizations like Doctors Without Borders, the International Red Cross, and so forth. At this stage, there are no antiviral drugs available and no vaccine, though there are active research programs in several institutions, including the US NIH Vaccine Research Center in Bethesda, Maryland. Though there is no product currently available, it would be a big plus if all African healthcare workers could be vaccinated against Ebola. Apart from develop specific “small molecule” drugs, monoclonal antibodies (mAbs) that bind to proteins on the surface of the virus may be useful for emergency treatment and to give those in contact “passive” protection for three or four weeks. Such “miraculous mAbs” can now be developed and produced quickly, though they are very expensive.
What is being done? Neighboring African countries are closing their borders. International agencies and governments are providing more professionals and other resources to help with treatment and tracking cases and contacts. Global companies have been withdrawing their workers and all nations are maintaining a close watch on air travelers who are arriving from, or have recently been in, these afflicted nations.
What is this Ebola catastrophe telling us? In these days of global cost-cutting, we must keep our National and State Public Health Services strong and maintain the funding for UN Agencies like the OIE, the WHO, and the FAO. High security laboratories (BSL4) at the CDC, the NIH and so forth are a global resource, and their continued support along with the training and resourcing of the courageous, dedicated physicians and researchers who work with these very dangerous pathogens, is essential. Humanity is constantly challenged by novel, zoonotic viruses like Ebola, Hendra, Nipah, Sin Nombre, SARS, and MERS that emerge out of wildlife reservoirs, with the likelihood of such events being increased by extensive forest clearing, ever increasing population size and rapid air travel. We must be indefatigably watchful and prepared. Throughout history, nature is our worst bioterrorist.
Peter C. Doherty has appointments at the University of Melbourne, Australia, and St Jude Children’s Research Hospital, Memphis. He is the 2013 author of Pandemics: What Everyone Needs to Know, which looks at the world of pandemic viruses and explains how infections, vaccines and monoclonal antibodies work . He shared the 1996 Nobel Prize for Physisology or Medicine for his discoveries concerning “The Cellular Immune Defense”.
What Everyone Needs to Know (WENTK) series offers a balanced and authoritative primer on complex current event issues and countries. Written by leading authorities in their given fields, in a concise question-and-answer format, inquiring minds soon learn essential knowledge to engage with the issues that matter today.
Subscribe to the OUPblog via email or RSS.
Subscribe to only health and medicine articles on the OUPblog via email or RSS.
The post How threatened are we by Ebola virus? appeared first on OUPblog.

With the Ebola virus in the news recently, you may be wondering what actions you can take to reduce the risk of contracting and spreading the deadly disease. Expert Peter C. Doherty provides valuable pointers on the best ways to stay safe and healthy in this excerpt from Pandemics: What Everyone Needs to Know answering: Is there anything that I can do personally to limit the possibility of a dangerous pandemic?
While pandemics are by their nature unpredictable, there are some things worth considering when it comes to the issue of personal safety and responsibility. The first point is to be a safe international traveler so that you don’t bring some nasty infection home with you. Protect yourself and you protect others. Though taking the available vaccines won’t prevent infection with some novel pathogen, it will contribute toward ensuring that you enjoy a successful vacation or business trip, and it should also put you in a “think bugs” mind-set. If, for instance, you are off to Africa for a wildlife safari, make an appointment at a travel clinic (or with your primary care physician) two to three months ahead of time to check your vaccine status and, if needed, receive booster shots to ensure that your antibody levels are high. Anyone who is visiting a developing country should make sure that he or she has indeed received the standard immunizations of childhood. Adolescents and young adults are much more likely to suffer severe consequences if, for instance, they contract commonplace infections like measles or mumps that have, because of herd immunity, become so unusual in Western countries that a minority of parents reject the collective responsibility of vaccinating their kids. If you’re younger and your parents are (or were) into alternative lifestyles, it may be wise to ask them very directly about your personal immunization history.
It’s also likely that, even if you were vaccinated early on, your level of immunity will have declined greatly and you will benefit from further challenge. Both possibilities will be covered if you go to a comprehensive travel clinic, as the doctors and nurses there will insist that you receive these shots (or a booster) if you don’t have a documented recent history. Any vaccination schedule should ideally be completed at least 3 to 4 weeks ahead of boarding your flight, the time needed for the full development of immunity. But this is one situation where “better late than never” applies. Should it have slipped your mind until the last minute, you should be vaccinated nevertheless. Even if you’ve never had that particular vaccine before, some level of protection could be there within 5 to 10 days, and a boosted, existing response will cut in more quickly. A travel clinic will also sell you a Gastro (gastroenteritis, not gastronomy) kit containing antibiotics to counter traveler’s diarrhea (generally a result of low-grade E. coli infection), something to decrease intestinal/gastric motility (Imodium), and sachets of salts to restore an appropriate fluid balance.
For the elderly, be aware of the decline in immunity that happens with age. You may not respond to vaccines as well as those who are younger, and you will be at greater risk from any novel infection. Depending on your proposed itinerary, it may also be essential to take anti-malarial drugs, which generally have to be started well ahead of arrival. Malaria is not the only mosquito-borne threat in tropical countries, so carry a good supply of insect repellant. In general, think about when and where you travel. Avoiding the hot, wet season in the tropics may be a good idea, both from the aspect that too much rain can limit access to interesting sites and because more standing water means more mosquitoes. Wearing long trousers, long-sleeved shirts, and shoes and socks helps to protect against being bitten (both by insects and by snakes), while also minimizing skin damage due to higher UV levels. Then, before you make your plans and again prior to embarking, check the relevant websites at the CDC, the WHO, and your own Department of Foreign Affairs (Department of State in the United States) for travel alerts. Especially if they’re off to Asia, many of my medical infectious disease colleagues travel with one or other of the antiviral drugs (Relenza and Tamiflu) that work against all known influenza strains. These require a prescription, but they’re worth having at home anyway in case there is a flu pandemic. If that happens, the word will be out that influenza is raging and stocks in the pharmacies and drugstores will disappear very quickly. But don’t rely on self-diagnosis if you took your Tamiflu with you to some exotic place; see a doctor. What you may think is flu could be malaria.
For those who may be sexually active with a previously unknown partner, carry prophylactics (condoms) and behave as responsibly as possible. Excess alcohol intake increases the likelihood that we will do something stupid. Dirty needles must be avoided, but don’t inject drugs under any circumstances. Blood-borne infections with persistently circulating viruses (HIV and hepatitis B and C) are major risks, while insect-transmitted pathogens (dengue, Chikungunya, Japanese B encephalitis) can also be in the human circulation for 5–10 days. Apart from that, being caught with illegal drugs can land you in terrible trouble, particularly in some Southeast Asian nations. No matter what passport you carry, you are subject to the laws of the country. Be aware that rabies may be endemic and that animal bites in general can be dangerous.
Can you really trust a tattooist to use sterile needles? Even if the needles are clean, what about the inks? How can they be sterilized to ensure that they are not, as has been known to occur, contaminated with Mycobacterium chelonae, the cause of a nasty skin infection? And that was in the United States, not in some exotic location where there may be much nastier bugs around.
Peter C. Doherty is Chairman of the Department of Immunology at St. Jude’s Children’s Research Hospital, and a Laureate Professor of Microbiology and Immunology at the University of Melbourne. He is the author of Pandemics: What Everyone Needs to Know, The Beginner’s Guide to Winning the Nobel Prize: Advice for Young Scientists, Their Fate is Our Fate: How Birds Foretell Threats to Our Health and Our World, and A Light History of Hot Air.
What Everyone Needs to Know (WENTK) series offers a balanced and authoritative primer on complex current event issues and countries. Written by leading authorities in their given fields, in a concise question-and-answer format, inquiring minds soon learn essential knowledge to engage with the issues that matter today. Starting July 2014, OUPblog will publish a WENTK blog post monthly.
Subscribe to the OUPblog via email or RSS.
Subscribe to only health and medicine articles on the OUPblog via email or RSS.
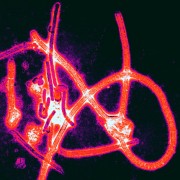
Image credit: Ebola virus particles by Thomas W. Geisbert, Boston University School of Medicine. Public Domain via Wikimedia Commons.
The post Limiting the possibility of a dangerous pandemic appeared first on OUPblog.




